
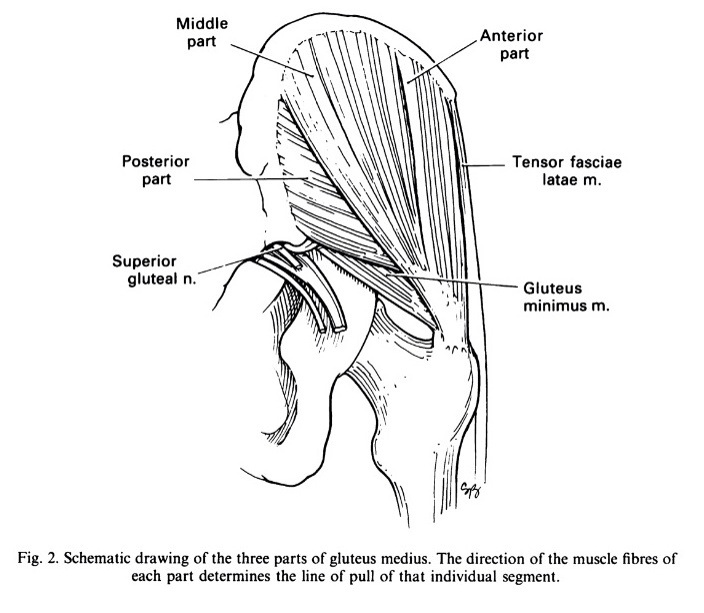
Over the last few months I have seen, what only could be called , an epidemic of glut med pain. So why? Like everything I think I may just see trends after they are too late to do anything about.So what is it and why is it appearing now In such numbers? One of the most common causes of hip pain is inflammation and degeneration of the glut med tendon and associated bursae. The Glute med (gluteus medius) is a deep hip muscle on the lateral aspect of the hip, that functions to stabilize the hip and control hip motion, particularly in weight bearing. The main issue with detecting that this is where the pain is, firstly to palpate properly and accurately over the correct muscle group, and then to test the muscle through the whole of the active ROM. Remember that glut med changes its function as the hip goes into flexion. If you test glut med in just one part of the the ROM, i.e. just where you would do a CLAM, you are missing the main functional parts of the ROM. Glut med controls the hip the whole way thought flexion, so should be tested functionally in this way.
If you think of the subjective and objective complaints of pain they are normally….
*Pain on laying on the side at night, pain on climbing hills or stairs increasing pain on walking on rough ground.
*If the patients over pronate then they are more susceptible to this injury as the knee falls inwards, increasing the Q angle at the hip, putting more load on the lateral hip muscles.
* Weakness in the hip abductors, especially gluteus medius has the same effect.
* Tight structures surrounding the hip such as the ITB, hip flexors and hamstrings as this causes biomechanical inefficiency and increased strain on the hip stabilizers. These maybe not tight but functionally overworking or patterning poorly.
* Look at the ROM at the Great toe… If they have a hallux rigidus then they will toe off laterally, not using the high gearing mechanism of the foot, and toe off in a pattern of least resistance. This can give a circumducting gait pattern and poor alignment in the push off phase.
* Women are more susceptible due to a naturally increased angle
between the hip and the knee, therefore increased load on the
glute med and other hip stabilizers.
Listening to what the exact aggregating factors are,putting the patient into that pattern of movement and analysing the whole of the kinetic chain are key to solving the problem.
